1 About this document
This document is for GP practice staff and clinicians and is intended as a brief guide to understanding and using Read Terms in practice. We only refer to Read Version 2, 5 byte as this is the version in use in GP systems in NHS Scotland.
2 What are Read Terms?
Read terms are a set of clinical descriptions that practices can use to manage the data in patients’ records. They are named after Dr James Read, the initial author of the terms.
The ‘Read terms’ refers to the words – the descriptions such as ‘Asthma’. Each term is associated also with a ‘Read Code’ – this is the letter and number code that uniquely identifies the clinical term. This can be up to five characters long, including full stops. For example, the Read Code ‘H33..’ is associated with the Read Term ‘Asthma’.
Read Codes can be used by computer systems for searching, reporting and decision support and allow data to be shared reliably between different computer systems.
3 How Read Terms are organised
3.1 Chapters
Read terms are organised by Chapters starting at Chapter 0 (zero), which contains terms for occupations, through to Chapter 9, and then chapters A to Z. The image below is from INPS Vision and shows this arrangement:
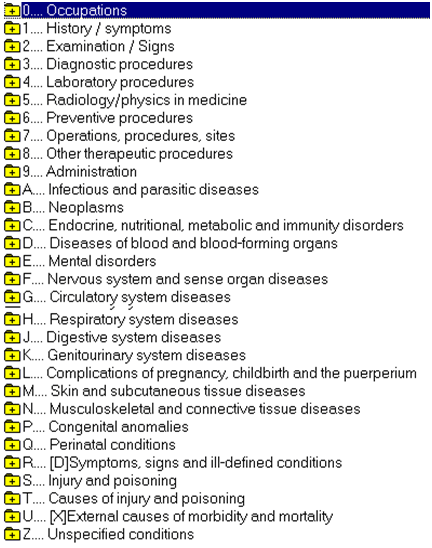
3.1.1 Chapter 0 – Occupations
The ‘0’ (zero) chapter contains terms used to describe occupations.
3.1.2 Chapters 1 to 9 – History, Examination, Procedures and Administration.
Chapter 1 contains terms useful in recording the patient’s history – symptoms, presenting complaints and past history. Chapter 2 has terms for recording examinations. Chapters 3, 4 & 5 allow the recording of investigations and tests. Chapter 6 contains preventative procedures such as screening and chronic disease monitoring. Chapter 7 provides terms for recording operations. Chapter 8 has terms for recording other therapeutic procedures such as physiotherapy, counselling and referrals. Chapter 9 contains terms useful for recording administrative procedures such as recording reports and certificates.
In general for most day to day activities of general practice Chapters 1 to 9 are the most useful – they contain terms that allows the practice to record the things it is doing every day and to manage its work and business.
3.1.3 Chapters A to U – Conditions, diagnoses, injuries
From Chapter A onwards the Read Terms are for recording disorders – diseases, conditions, injuries. These are sorted into chapters based on system (e.g. Respiratory) or cause (e.g. Congenital).
3.1.4 Chapter Z – Unspecified conditions
This chapter is for completeness and links to ICD-10 – the coding system used mostly in secondary care. It contains terms to record “Supplementary factors influencing health status or contact with the Health services other than for illness”. In general its usefulness in general practice is limited.
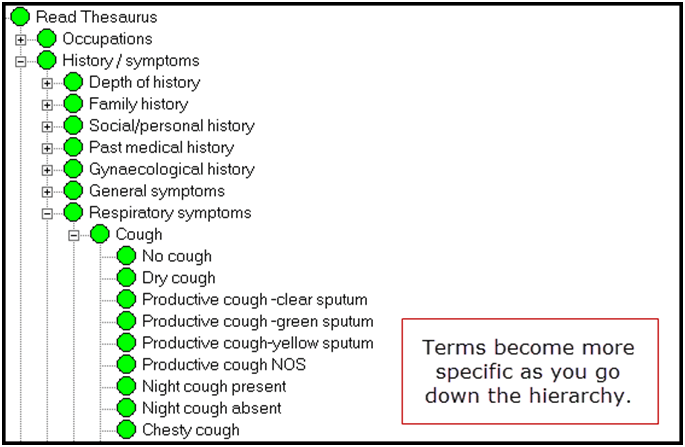
3.2 Hierarchical
Within the chapters terms are organised hierarchically, that is moving from more general terms to more specific terms as you move down the hierarchy.
Generally the Read Code is incrementally increased as you move down the hierarchy. For example:
| 1…. History / symptoms |
| 17… Respiratory symptoms |
| 171.. Cough |
| 1714. Productive cough -green sputum |
Organising the Read Terms like this makes it easier to find an appropriate term – users can drill down into Read Hierarchy to find the most specific term they can for any given clinical concept. It also makes it easier to search and report on stored data. For example, a computer can find all patients with respiratory conditions by looking for records that contain any codes beginning with ‘H’, or all patients with a record of cough by looking for records that contain codes beginning with ‘171’.
3.3 Absence or ‘Negation’ – aim to be specific
The Read terms do not always manage to make it easy to say that a particular condition or event is not present or did not happen. This is because often the first Read Term in a hierarchy may be the Term stating that the condition is not present. As above, the first term after ‘Cough’ is ‘No Cough’.
This has the effect of complicating searches. Users of Read Terms can reduce this complexity by trying to use the most specific and appropriate Term for any condition by selecting a term lower down the hierarchy whenever possible.
3.4 Abbreviations
Read Terms often have abbreviations or prefix letters associated with them. These have different meanings and it is helpful to have some understanding of them.
3.4.1 ‘NOS’ – Not Otherwise Specified
This is a common abbreviation in many parts of Read. It should be used when no other clinical term is available that is more specific or accurate for describing the concept you are trying to record.
By way of illustration: for cough with sputum, as shown above, there are specific terms for ‘Clear’, ‘Green’ and ‘Yellow’ but if your patient was complaining of ‘Grey’ sputum, or ‘Frothy’ sputum then the term ‘Productive Cough NOS’ would be appropriate.
3.4.2 ‘NEC’ – Not Elsewhere Classified
This refers to Read Terms which appear only in one place – that is the same clinical concept is not available to be recorded in a better way in a different part of Read. This can occur where a condition may have different classifications – such as neurological conditions that are caused by infections – and so could be represented in different ways in different chapters. In practice this does not matter significantly, and unless you think there may be a better chapter in which to find an appropriate code it is often reasonable to use the ‘NEC’ term.
3.4.3 Chapter R – ‘[D]’ Terms
The terms in Chapter R are defined in the Read Thesaurus as ‘Symptoms, signs and ill-defined conditions.’
In general practices should avoid using these terms as they are often vague and non-specific. Normally when trying to find the best Read Term for a disease or disorder the other disorder chapters are more appropriate. Better and more comprehensive symptoms and signs terms are available in Chapters 1 and 2.
There are occasions, however, where a symptom or sign is considered significant enough to record as a disorder, or where it is the only presentation of the disorder. For example, where a patient complains of chest pain but, after investigation, no cause is found it may be appropriate to use the term “R065. [D]Chest pain” to record it as a disorder. For recording the symptom of chest pain chapter 1 terms of ‘182..00 Chest pain’ or below would be more appropriate.
3.4.4 7N…Subsidiary classification of laterality and operation sites – ‘[SO]’ – ‘Site of’
Chapter 7 describes terms for Operations, Procedures and Sites. The section under 7N contains terms for describing the site of an operation (e.g. Appendix) – this does not describe the actual operation or procedure itself (i.e. Appendectomy). In general practices should avoid using the terms prefixed with ‘[SO]’.
3.4.5 BB… ‘[M]’ – Morphology of neoplasms
Chapter B contains terms for recording the diagnosis of Neoplasms. Chapter BB contains terms that describe the neoplasm’s morphology not the actual diagnosis. Unless specifically recording the morphology of a neoplasm, practices should avoid using terms prefixed with ‘[M]’.
3.4.6 14… Past Medical History ‘H/O’ Terms – ‘History Of’
These terms are prefixed with ‘H/O’ and can be used to record the patient’s reported past medical history, or where noting that a clinician is aware of the past condition. For example: if during a consultation the patient states they have ‘Diabetes’, the user may wish to note this and code it as ‘1434. H/O: diabetes mellitus’, but the record of the condition would still need to be added separately using the actual date of onset and a code from the section ‘C10.. Diabetes mellitus’.
‘H/O’ terms do not code disorders and the actual condition needs to be recorded using a term from Chapter A or later. Do not use ‘14… H/O’ codes for recording important summary items.
3.4.7 12…00 Family history – ‘FH’
Terms prefixed ‘FH’ in chapter ‘12…’ refer to the patient’s reported or known family history and do not indicate the patient themselves has the disorder.
3.4.8 ‘[X]’ Prefix
These terms, such as those under ‘Eu…00 [X]Mental and behavioural disorders’, have an ‘[X]’ prefix. This simply means that the term has an equivalent code in ICD-10, the hospital coding system. The terms themselves are reasonable to use for recording disorders in primary care, the ‘[X]’ prefix is irrelevant for our purposes.
3.5 Synonyms or ‘Term Codes’
Sometimes there is more than one way of describing the same clinical concept. For example, a ‘Myocardial Infarction’ may be referred to as a ‘Heart Attack’. In Read Terms this is managed by having a ‘Preferred Term’ – the one that Read would like you to use – and ‘Synonyms’ (sometimes called ‘Term Codes’) that are different text descriptions of the same thing. For example some of the synonyms for ‘G30..’ are:
| Read Code | Term Code | Term | |
| G30.. | 0 | Acute myocardial infarction | Preferred Term |
| G30.. | 11 | Attack – Heart | Synonym |
| G30.. | 12 | Coronary Thrombosis | Synonym |
| G30.. | 14 | Heart attack | Synonym |
| G30.. | 15 | MI – Acute Myocardial Infarction | Synonym |
3.5.1 Incorrect Synonyms
Over time some synonyms have been added to Read Terms that have a different meaning from the preferred term. For example, one of the synonyms for ‘G30..’ is:
“G30..13 Cardiac rupture following myocardial infarction (MI)”
This is simply incorrect as it is a different condition from the Preferred Term. Use of such synonyms where their meaning is different from the preferred term should be avoided. Wherever possible use the Preferred Term.
3.6 Avoid changing meaning in free text
Users should never change the meaning of a Read Term with associated free text. For example, entering the code:
“G30.. Acute myocardial infarction”
and then appending a free text comment of ‘Absent’ or ‘Negative’.
The presence of the code ‘G30…’ in the patient’s record will effectively state they have had a Myocardial Infarction when viewed elsewhere or used for reporting and decision support.
3.7 Use the correct term in the hierarchy
It is essential that people adding clinical terms can understand their meaning in the context of the Read hierarchy. For example, entering the term ‘A98z. Gonorrhoea’ effectively states that the patient has had this condition. It should not be used as a proxy for a test for Gonorrhoea, thus appending free text of ‘Negative’ will not, in computer terms, indicate the intended meaning. A user entering a test result must understand where in the hierarchy to look in order to avoid this type of error. In this instance the correct term would be “4JQ8. Gonorrhoea test negative”.
3.8 Local codes in EMIS
Users of the EMIS clinical system may be aware of various “local codes” that exist on the system. Local codes are not Read Codes so cannot be reliably shared across different computer systems. In the PCS application the following may exist on the system
- Codes of the form ‘EMISxxxxx’
- Codes of the form ‘EGTONxxxx’
Both the above are the same on any EMIS system, but should not be used as there is usually a reasonably similar Read code or something that might be made to approximate.
- Codes of the form ‘PCSDTnnnnn_ccc’ where ‘nnnnn’ is the EMIS CDB number of the site and ‘ccc’ is the code number:; these are used to represent items that came over from a previous clinical system and have not (yet) been mapped to an appropriate read code. This type of code has no meaning outside the originating site.
e.g. PCSDT19213_122 HbA1c date
- Codes of the form ‘PCSnnnnnaac’ where ‘nnnnn’ is the EMIS CDB number of the site, ‘aa’ is the first 2 letters of the code description, and ‘c’ is a number; these are local codes consciously created by the practice. This type of code has no meaning outside the originating site.
e.g. PCS19213SP1 SPSP Outpatient Action